
by admin | Aug 4, 2025 | Custom Content, Employee Benefits
Employers will see several changes to their health and welfare benefits due to comprehensive new tax and spending legislation. This includes notable improvements to Health Savings Accounts (HSAs), Dependent Care Flexible Spending Arrangements (DCFSAs), and employer-provided student loan payments, as well as the introduction of some new fringe benefit choices.
These updates introduce significant changes to employee benefits. These changes are part of a comprehensive legislative package enacted on July 4, 2025 and will require employers and employees to adjust their understanding and utilization of benefit programs. Some of the most notable provisions are:
- Health Savings Accounts (HSAs) can now cover Direct Primary Care (DPC) fees, up to $150/month for individuals and $300/month for families.
- The telehealth exception for high-deductible health plans (HDHPs) is now permanent, ensuring continued access to virtual care. Employees with HDHPs will have first-dollar coverage of most telehealth services, before meeting their HDHP deductible.
- The dependent care FSA limit has increased from $5,000 to $7,500 ($3,750 for married filing separately), a boost for working parents.
- Bronze and catastrophic ACA exchange plans are now HSA-qualified.
- The tax exclusion for employer-sponsored health insurance remains intact, a win for traditional group benefits.
- Permanent exclusion for student loan assistance allows for a tax exclusion of up to $5,250 per year for employer payments of student loans and offers long-term support for employees managing student debt.
- New tax-advantaged accounts for children (a.k.a. “Trump Accounts”) are individual retirement accounts (IRAs) for children under 18 with an annual contribution cap of $5,000. These accounts allow for employers to contribute up to $2,500 per employee. Additionally, children born between January 1, 2025, and December 31, 2028, are eligible to receive a one-time $1,000 government contribution.
These changes are important as they significantly impact the employee benefits landscape. They also enhance access to care, reduce wait times, and provide greater flexibility, cost savings, and options for both employers and employees. By leveraging these updates, organizations can elevate employee well-being while remaining tax-compliant and strategically competitive.

by admin | Jul 28, 2025 | ACA
Big changes are coming to women’s preventive care coverage! Starting with plan years on or after December 31, 2025, group health plans and health insurance issuers must expand their no-cost coverage for women’s preventive care. This expansion includes additional breast cancer imaging or testing needed to complete an initial mammogram, as well as patient navigation services for breast and cervical cancer screenings.
These updates fall under the Affordable Care Act’s (ACA) preventive care mandate, which requires most health plans to cover a range of preventive services without deductibles, copayments, or coinsurance when using in-network providers. The ACA’s guidelines are regularly updated.
The latest HRSA-supported guidelines, updated on December 30, 2024, specifically expand breast cancer screening to include necessary follow-up imaging (such as MRIs or ultrasounds) or pathology evaluations beyond the initial mammogram. Additionally, starting in 2026, patient navigation services for breast and cervical cancer screening and follow-up will be covered. These services offer personalized support, help with healthcare access, referrals to essential services (like language translation or transportation), and patient education.

by admin | Jul 23, 2025 | Human Resources
When considering employee retention, HR professionals must realize that turnover doesn’t begin with a resignation letter. It starts much earlier—and it’s quieter. A skipped lunch, a missed meeting, fewer Slack messages. These small signs often signal something much bigger: an employee pulling away. Long before someone quits, they disconnect. And in today’s networked workplace, social withdrawal is often the first—and most reliable—indicator that someone’s already halfway out the door.
While voluntary turnover has dropped to 13.5 percent—a sharp decline from 24.7 percent in 2022—that doesn’t mean employees are engaged. According to Gallup, more than half of U.S. workers are either actively searching or watching for new jobs. One in three say they’re ready to quit—even without something else lined up. This isn’t just dissatisfaction. It’s detachment. And it’s quietly reshaping our workforce.
Gallup calls this the “Great Detachment.” Employees are still showing up—but they’ve stopped buying in. They’re physically present, but relationally and emotionally checked out. And if left unchecked, this detachment becomes the precursor to departure.
Employee retention: Why people leave before they leave
Network analysis has consistently identified one of the most powerful—and overlooked—predictors of employee turnover: social isolation. While compensation, career mobility, and flexibility certainly matter, they rarely tell the whole story. People don’t just leave because of what they’re missing in their role. They leave because of what they’re missing in their relationships. When employees feel disconnected from their peers, excluded from informal conversations, or cut off from trusted collaborators, a sense of belonging erodes. And once that sense of belonging fades, disengagement—and eventual departure—often follows.
Employees on the edge of the network—those with limited connections—are two to three times more likely to quit. Without strong ties, they’re often left out of critical conversations, informal support, and growth opportunities. In fact, disengagement typically begins at the edges, long before it shows up anywhere else.
But a new pattern is emerging inside organizations: some employees aren’t just stuck on the edges—they’re choosing to move there. They’re intentionally stepping back from collaboration, reducing their interactions, and moving to the periphery of the network by design rather than by default.
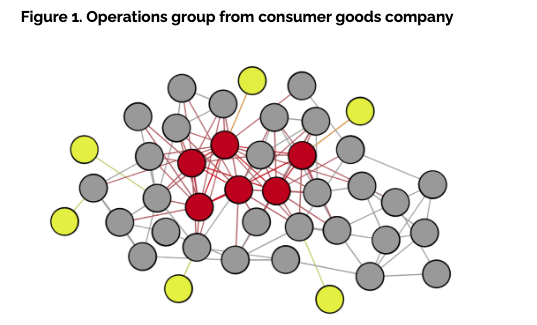
Just consider the organization below, it represents an operations group of just over 40 employees within a global consumer goods company, a network analysis revealed a disturbing trend. Six employees—represented in yellow nodes (Figure 1)—were only connected to one other colleague. Several more had just two connections. And while that level of isolation is concerning on its own, what made it worse was that nearly half of these individuals were previously well-connected just a year earlier. They hadn’t just become isolated. They had chosen to pull back.
A recent study from Thred provided even more compelling evidence: employees who had recently resigned had 36 percent fewer connections than the company average. Even more telling, they were twice as likely to report having no meaningful friendship relationships at work. These findings point to a deeper insight—relational connectedness is more than a cultural asset; it’s a predictive signal. Building strong interpersonal ties may be one of the most underutilized levers in improving employee retention.
The contagious nature of the center
Research has long shown that employees at the center of an organizational network—those with many active connections—are 24 percent less likely to leave. These individuals, much like the red nodes in Figure 1, are deeply embedded and often serve as the glue that holds teams together. Their centrality provides access to information, influence and support.
And when those connections go beyond the professional—when they include genuine friendships—their likelihood of staying increases even more. Research has found that employees engaged in dual-purpose relationships—blending both professional collaboration and personal rapport—were 37 percent less likely to quit than those with purely transactional ties. When relationships go beyond the task at hand, people are more likely to stay—not just for the work, but for the sense of shared connection.
But here’s where it gets more complex. When well-connected, central employees become burned out, disengaged or disillusioned with the organization’s direction, their influence can shift from stabilizing to destabilizing. According to Thred’s research, when a central employee leaves, as much as 25 percent of their immediate network is likely to follow within months. These aren’t isolated exits—they’re relational chain reactions.
In highly collaborative environments, the ripple effect of a single departure can quickly cascade across a team. Employees who leave often hold more than just a role—they serve as connectors, mentors and informal leaders whose influence stretches far beyond their job title. When they exit, it disrupts not only workflows but the underlying trust networks that hold teams together. Like a contagion, quitting spreads through connection: the closer someone is to a departing colleague, the more likely they are to re-evaluate their own sense of belonging, purpose, and place within the organization.
The effect can cascade across teams, departments and even geographies—especially in highly collaborative organizations. Like a virus, quitting spreads through proximity. The closer you are to someone who leaves, the more likely you are to consider it too.
What HR can—and should—do
For HR leaders, the implications are clear: employee connection is no longer a soft metric. It’s a strategic one. The good news? Relationships are something organizations can influence—with intention.
Here are four high-impact ways to foster friendship—and reduce attrition:
1. Use network analysis to spot flight risk early
Conduct regular organizational network analysis to identify employees with few or declining connections. These individuals are not just disengaged—they’re already on their way out. Early detection can inform re-engagement strategies or personalized outreach. And if you can’t run an analysis, just watch. Notice who is leaning back more often than they used to.
2. Facilitate moments of connection
Friendship doesn’t form by accident—especially in hybrid or remote settings. Use tools like interest-based matching (for example, Thred’s Stitches) to facilitate meaningful one-to-one meetups. Host curated mixers, team swaps or mentorship pairings that prioritize human connection, not just transactional interactions.
3. Support relationship-rich teams
Encourage cross-functional initiatives where both personal rapport and professional trust can develop. Invest in psychologically safe team cultures that allow for vulnerability, shared experience and the blending of professional and personal interest.
4. Routinely pulse check with central employees
Central employees with high trust capital have the greatest influence on the network. If they’re thriving, they’ll lift others with them. But if they’re frustrated or burned out, their exit could trigger a talent drain. Keep these employees close—and engaged.
By Michael Arena
Originally posted on HR Exchange Network

by admin | Jul 15, 2025 | Custom Content, Employee Benefits
Want to attract and keep top talent? Your benefits package is crucial! Think beyond just health and retirement. Fringe benefits like Dependent Care Assistance Programs (DCAPs) offer real, meaningful support, especially for employees caring for kids or dependent adults.
What is A DCAP?
A DCAP – also known as a dependent care flexible spending account (DCFSA) (since it functions similarly to a health flexible spending account (FSA)) – helps to ease the financial burden. This program allows employees to set aside pre-tax dollars specifically for eligible dependent care expenses, providing a substantial financial advantage. Through convenient payroll deductions, employees contribute pre-tax funds to this account. These funds can then be used to reimburse them for qualifying expenses such as daycare, babysitting services, or after-school programs.
DCAPs can be standalone benefits or part of a larger “cafeteria plan.” Regardless, they operate under strict IRS rules to ensure proper use of the funds.
What Expenses Qualify for Reimbursement?
To qualify for reimbursement, the expense must be directly related to care that enables the employee (and their spouse, if applicable) to work or look for work. Reimbursement is provided after the care has been rendered.
Eligible Expenses Include:
- Preschool, nursery school, or similar programs (below kindergarten level).
- Before- and after-school care for children.
- Day camps, including specialized camps (e.g., sports, computer).
- Transportation to and from the place of care, if provided by the care provider.
- Employment taxes paid to a caregiver.
- Room and board for a caregiver (in specific cases).
- Application or agency fees related to finding care.
Ineligible Expenses Include:
- Kindergarten tuition or higher education costs.
- Overnight camps.
- Payments made to an employee’s spouse or the child’s other parent (if not their spouse).
Who Qualifies as a Dependent?
Employees can utilize DCAP funds for:
- A dependent child under the age of 13.
- A spouse or dependent who lives with the employee and is physically or mentally unable to care for themselves.
It is important for employees to note that eligibility is calculated on a daily basis. For example, reimbursement cannot be sought for expenses incurred after a dependent’s 13th birthday.
Contribution Limits
Internal Revenue Code Section 129 sets annual contribution limits for DCAPs, ensuring tax compliance:
- Up to $5,000 per year for employees who are single or married filing jointly.
- Up to $2,500 per year for employees who are married filing separately.
These pre-tax contributions are a significant advantage, reducing an employee’s taxable income and thereby increasing their take-home pay. It’s also important for employees to understand that the same expenses cannot be claimed for both a DCAP and the federal dependent care tax credit.
DCAP contributions must be used for eligible care expenses within the coverage period, or they are forfeited. This is often referred to as the “use it or lose it rule.” While a 2.5-month grace period for incurring and submitting claims is permitted, DCAPs do not allow carryovers of unused funds to the next plan year. Additionally, a DCAP is not portable – meaning that if an employee leaves, the funds are forfeited.
Maximizing Benefits for Employees
Offering a DCAP provides meaningful support to employees, whether they are new parents, caring for a loved one with special needs, or simply seeking ways to manage household budgets more effectively. It is a valuable tool that helps team members save money while managing essential care costs.
by admin | Jun 30, 2025 | Custom Content, Employee Benefits
Selecting the right health insurance plans for your family is a critical process that requires careful attention from start to finish. Navigating health insurance becomes much simpler when you understand its terminology. Making sense of these terms empowers you to better understand your costs, benefits, and even estimate the price of a doctor’s visit.
Premium: Your Insurance Payment: The premium is the regular payment you make to an insurance company to maintain your coverage. When you get insurance through your employer, they will specify how much of the premium you are responsible for, and this amount is typically deducted from your paycheck before your taxes are calculated.
Copayment : A copayment, often called a copay, is a specific amount you pay for a covered healthcare service, and it’s usually due when you receive that service. The amount of the copay can be different for different types of care.
Copay Example: For her son’s pediatrician visit for the flu, Heather had a $15 copay that she paid at the time of the appointment.
Deductible: A deductible is the amount you pay for healthcare services each year before your insurance starts covering costs.
Deductible Example: Ashley has a $1,000 annual deductible. Her first arm surgery costs $800. Since she hasn’t met her deductible yet, she pays the full $800.
Coinsurance: Coinsurance is the percentage of the allowed cost for a covered healthcare service that you’re responsible for paying after you’ve paid your deductible.
Coinsurance Example: Ashley’s next surgery costs $3,200 (the allowed amount). She has already paid $800 of the $1,000 deductible so she is responsible for the first $200 of the second surgery. Her insurance has an 80/20 coinsurance split. This means they pay 80% ($2,400), and Ashley pays 20% ($600).
Out-of-Pocket Maximum (OOPM): The OOPM is the maximum amount you’ll pay for covered healthcare costs in a year, not counting your monthly premium. It acts as a financial safety net against very expensive medical care. After you reach your yearly OOPM, your insurance pays 100% of covered costs for the rest of the year. Be aware that some plans have rules about what expenses count towards your OOPM; for instance, some might not include your deductible.
OOPM Example: Ashley has a $3,000 out-of-pocket maximum and has paid $1,600 so far. Her next surgery costs $8,000. She will pay her 20% coinsurance until her total out-of-pocket reaches $3,000. She has $1,400 left to pay. After that, her insurance covers the remaining $6,600.
Preventive Care: Preventive care focuses on staying healthy and catching illnesses early. It includes medical tests, vaccines, screenings, and medications designed to prevent chronic diseases. The goal is to identify and treat health issues in their most manageable stages. Under the Affordable Care Act (ACA), most health insurance plans must cover a range of preventive services without charging copays, deductibles, or coinsurance.
Preventive Care Example: Lori makes an appointment for her yearly check-up and a mammogram with a doctor in her network. Since these are preventive services covered by the ACA, Lori pays nothing – her health insurance covers the full cost.
Other Benefits Terminology
Pre-existing Condition: This is any health issue (physical or mental, including disabilities) you had before your health plan started. Since 2014, most insurers can’t deny coverage or charge more for pre-existing conditions, unless you have a “grandfathered” plan.
Grandfathered Plan: This is a health plan that existed before the ACA (2010) and hasn’t changed much since. These plans don’t have to follow all of the ACA’s rules.
Summary of Benefits and Coverage (SBC): The SBC is a straightforward document that outlines the costs and coverage of a health plan in an easy-to-compare format.
All those healthcare acronyms and terms might seem overwhelming but taking the time to learn them can put you in control. Understanding the lingo makes it easier to pick a health plan that meets your individual needs and budget!